
[MEETING HIGHLIGHTS]2022 Taiwan Expert Meeting: GH Treatment Optimization with Patient Journey, and the Combination Therapy
On October 23, 2022, we held the “Taiwan Pediatric and Endocrinology Expert Meeting: GH Treatment Optimization with Patient Journey” and invited pediatric metabolic endocrinologists to discuss the content and treatment of growth hormone therapy.
Background
Since October 2020, the Taiwan Precision Child Health Association (TPCHA) has been interviewing experts throughout Taiwan to discuss the issue of short stature in children. Last year, Taiwan’s top experts were invited to discuss the duration of the treatment along with the suitability of the patient. The definition of therapeutic response, the initial treatment dose, and the dose adjustment of idiopathic short stature (ISS) were also discussed. In the previous meeting, the experts reached a consensus. Additionally, an expert pointed out that if puberty began during the treatment of short stature, how long before epiphyseal closure, would it be appropriate to start the treatment? Physicians often nee d to consider bone age (BA) > chronological age (CA) and BA = CA in the treatment of short stature. The skeletal development often
involves, the development of early or precocious puberty, hormonal treatment, the combination ofgrowth hormone (GH) and gonadotropin-releasinghormone agonist (GnRHa), etc. In addition, someISS patients may also receive combined GH/GnRHatherapy.
This year we want to understand the views ofexperts on the use of combined GH /GnRHatherapy. Since April 2022, TPCHA has beeninterviewing a total of 17 experts in Taiwan (8 fromthe North, 6 from the Central, and 3 from theSouth) to discuss the following topics:
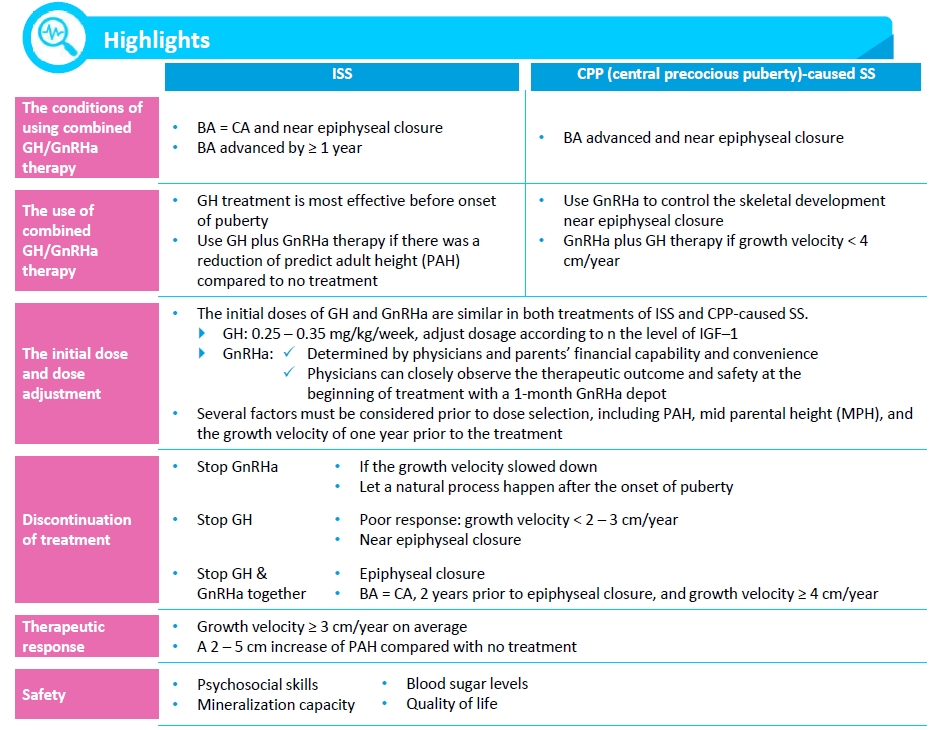
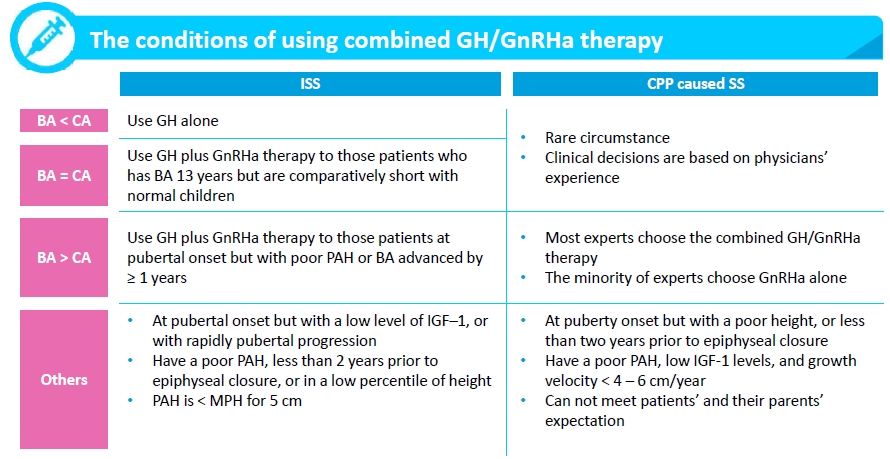
- The conditions of combined GH/GnRHa therapy
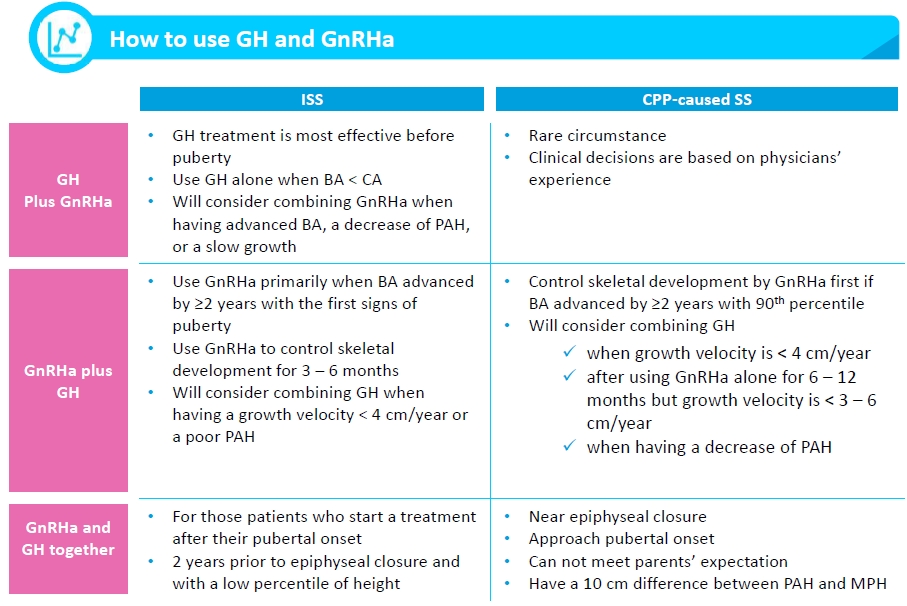
- The use of combined GH/GnRHa therapy
- The initial dose and dose adjustment
- Discontinuation of treatment
- Therapeutic response
- Safety
Literature reviews on combined GH/GnRHa therapy
For the treatment of CPP, experts in the advisory board meeting still maintain the consensus in 2009:historical series of untreated patients reported mean heights of 152 cm in girls and 156 cm in boys, a lossof ~10 cm in girls and ~20 cm in boys. GnRHa may slow growth velocity since GnRHa leads to a decline inIGF-1 and IGFBP-3 ratio, which affects free IGF-1 concentration significantly[1] . Therefore, using GH is one ofthe options to promote growth outcomes. Studies have shown that combined treatment of GH and GnRHaleads to an increase of PAH by 4.7 – 8.2 cm[2] .
GnRHa treatment has been a standard of care in girls with progressive CPP. Some studies havesuggested that GH should be combined with GnRHa if PAH below the fifth percentile, growth velocity < 5cm/year in the first year of treatment, or the growth velocity at -1 SD. To treat patient with ISS, there is noconsensus of treatment of combined GH/GnRHa therapy. A study showed that there was a positive effectof GH/GnRHa therapy to the children who even near the end of puberty2 .
[1] Müller J, et al. J Pediatr Endocrinol Metab. 2000 Jul;13.
[2] Bereket A. J Clin Res Pediatr Endocrinol. 2017;9(Suppl 2):33-48.
Expert Opinion
To consider combined GH/GnRHa therapy, experts have different criteria for theminimum PAH. The basic consensus is girls < 153 cm, and boys < 165 cm. Some expertsshowed concerns regarding using BA as the only standard to treat CPP.
All experts will not refer to the difference between PAH and MPH because of thelarge deviation of MPH. The physicians’ main considerations include tracking growthvelocity, parents’ needs, children’s motivation, lifestyle modification, etc. Most physiciansfirst look at the current patient’s condition and then decide on the appropriatetreatment. Physicians may consider combined GH/GnRH therapy actively if the patient’sgrowth velocity is < 3 cm/year. However, this therapy would not be used at the initial stage in general. The expert’s consensus is that early diagnosis will result in the mostpositive outcome.
Expert Opinion
For ISS children who first receive GH and then combine it with GnRHa treatment, theparticipating experts believe that these patients should meet the following criteria:
- Approaching puberty
- Growth velocity < 4 cm/year
- With accelerated BA or BA > CA
- Meet the parents’ expectations
- Parents have the financial means
Most physicians ask children to adjust their lifestyle to control the progression of puberty and skeletal development before treatment. An expert mentioned that it isnecessary to be careful with the treatment strategy and PAH is not the only criterion. When treating children with CPP, physicians control the progression of BA primarily. Thecombined GH therapy would be used if CPP children start puberty or GnRHa treatmentdid not meet the purpose.
Key consideration of combined GH/GnRHa therapy:
Puberty, Growth Velocity, Tracking BA, and parents’ expectations
The initial dose and dose adjustment
GH
Most physicians use similar initial doses of GH to treat patients with ISS or CPP-caused short stature.According to previous Taiwan-wide interviews, physicians chose an initial dose of 0.25 mg/kg/week onaverage (a range from 0.178 – 0.35 mg/kg/week). Most physicians use less than 0.35 mg/kg/week of GHat the highest dose. Physicians will adjust the dosage according to patient weight and monitor the level ofIGF-1 (with +2 SDS as the cut-off criterion).
Experts mentioned two ways of GH dose adjustment:
- Add 0.02 – 0.05 mg/kg/week each time
- Add 0.014 mg/kg/week each time
GnRHa
Most physicians use both dosage forms of GnRHa: 3.75 mg (1-month GnRHa depot) or 11.25 mg (3-month GnRHa depot). Physicians use a 1-month GnRHa depot for at least three months and then switchto a 3-month GnRHa depot after confirming patients remain in stable condition. Some experts feel thatthe 1-month GnRHa depot is better for tracking patients’ condition. A physician shared that the literaturehas confirmed that the therapeutic effect of a 1-month GnRHa depot is better because a higherfrequency of visits to the doctor has a positive effect on compliance. Some physicians prefer to use the 3-month GnRHa depot for saving patients’ time. Most experts will not adjust the dose of GnRHa unless thepoor response. There are three different ways of dose adjustment:
- Use a dose of 1.88 mg if the patient’s body weight is < 20 kg, and use a dose of 3.75 mg if thepatient’s body weight is ≥ 20 kg
- Keep a fixed dose and ask patients to control their weight
- Adjust treatment by shortening the interval between injections:
>> 1-month GnRHa depot: every three weeks
>> 3-month GnRHa depot: in ten to eleven weeks
Discontinuation of treatment
The literature indicates that patients with CPP who are diagnosed before the age of 6 can gain 9 – 10cm of height on average after treatment, and between the ages of 6 and 8 can gain an average of 4.5 – 7.2cm. For patients with early fast puberty (EFP), the combined therapy could improve the height by only 1cm[3].
There are two clinical observations: (1) the combined GH/GnRHa therapy can help patients increase2.8 – 4.3 cm compared with GnRHa alone, and (2) Receiving combined GH/GnRHa therapy for at least oneyear led to a significant increase in final height.
[3] Lazar L, et al. J Clin Endocrinol Metab. 2007;92:3483-9
Expert Opinion
Regarding combined GH/GnRHa therapy for ISS or CPP-caused SS, most physicians choose todiscontinue GnRHa first. Physicians prefer to use GH alone at the late stage since GnRHa mayslow growth velocity. 2 cm/year is the minimum expectation of growth velocity with GnRHatreatment. At least a growth velocity of 4 cm/year should be achieved if combined GH/GnRHatherapy is used. Additionally, physicians may also consider discontinuing GnRHa first if thepatient’s BA is advanced, or puberty is approaching. Most physicians want to let childrendevelop puberty naturally.
Some physicians consider discontinuing the use of GH and GnRHa together when epiphyseal closure. Some physicians choose to discontinue GH first due to poor response, such as a growthvelocity < 2 – 3 cm/year or growth plate closure. In addition, some physicians mentioned thatstopping GH first often occurs when treating ISS patients. Physicians may let children developnaturally after onset of puberty, or BA grows well and reaches the appropriate percentile. All physicians prioritize healthcare regulations and parental concerns.
Therapeutic response
Lifestyle and treatment timings are crucial to the effectiveness of the therapeutic response. Additionally,heredity, compliance, length of treatment, puberty, the child’s motivation, and parents’ financial capabilityhave also been mentioned by experts. According to studies, combined GH/GnRHa therapy has a betterprognosis, and the outcome will be more positive for those patients who receive the treatment before theage of 10. Research has also shown that with 2-year, combined therapy, boys are able to reach their MPH[4],[5],even though they started treatment after they were 12 or 13 years old. According to meta-analysis, for ISSpatients, individual differences exist in the therapeutic response of combined therapy[6].
[4] Wang M, et al. Sci Rep. 2016 Apr 13;6:24259.
[5] Li S., et al. Endocrine. 2020 Sep;69(3):615-624.
[6] Song W., et al. Int J Endocrinol. 2018 Dec 30;2018:1708650.
Expert Opinion
Growth velocity is primary criteria used to evaluate the effectiveness of thecombined therapeutic response. Physicians wish to see that there is at least 3 cm/yearof growth velocity on average (a range from 3 to 8 cm per year).
Experts also outline the following conditions which may affect the overall therapeutic response:
- Increase of PAH by 2-5 cm
- After combined therapy, BA gradually becomes BA closer to CA
- Does the outcome meet the parents’ expectations?
- Has the patient have received the treatment before the onset of puberty?
- Patients with good MPH usually have a better response to the treatment
Safety
Reaching the ideal height safely is the most important thing. There are some potential side effects ofthe combined GH/GnRHa therapy including weight gain, adverse effects on bone mineralization, andpsychological effects[7]. However, the current literature indicates that adverse effects on psychosocial functionhave not been found[8]. Some physicians suggest that blood sugar should also be monitored.
[7] Wit J M, et al. Eur J Endocrinol. 2004 Aug;151.
[8] Mauras N, et al. Endocr Rev. 2022 May 27;bnac014.
Expert Opinion
The safety profile of combined GH/GnRHa therapy was similar to the use GH and GnRHa alone. Since the
COVID-19 pandemic, physicians have found adverse events related to diagnosis or vaccines in clinical practice. Some experts shared that several patients had swelling around the eyes and lips after GnRHa administration. Patients with these acute allergic reactions have been both vaccinated and diagnosed with COVID-19. Physicians have suggested that it was possibly due to repeated systemic immune responses. There were also physicians who shared that patients’ menstrual cycles have been affected after being vaccinated, diagnosed with Covid-19, or taking NRICM101. As the pandemic is a new global challenge, physicians must pay more attention to clinical observation and treatment.
Conclusion
During the treatment, physicians need to understand the patient’s profile, their growth status, skeletaldevelopment, and puberty. The use of GH and GnRHa is decided by professional judgment, the financialcapability of the family, and the mental condition of patients. In conclusion, early treatment and along withthe appropriate dose intervention are positive for the improvement of height in children.
MODERATOR
Dr. Der-Ming Chu (TSGH)
Dr. Fu-Sung Lo (CGMH-LK)
Dr. Pen-Hua Su (CSMU)
SPEAKER
Dr. Chao-Hsu Lin (MMH-HC)
EXPERT (list in alphabetical order)
Dr. Chen Yang (IHMED / TMUH)
Dr. Chia Chi Hsu (VGHTC)
Dr. Chung-Hsing Wang (CMUH)
Dr. Ja Wei Hou (CGH)
Dr. Li-Ping Tsai (TZUCHI-TP) (online)
Dr. Mei-Hong Wen (BOAIHS)
Dr. Meng-Che Tsai (NCKU) (online)Dr. Yi-Ching Tung (NTU)
Dr. Yi-Shou Lin (TNHOSP)